
{kind=link}
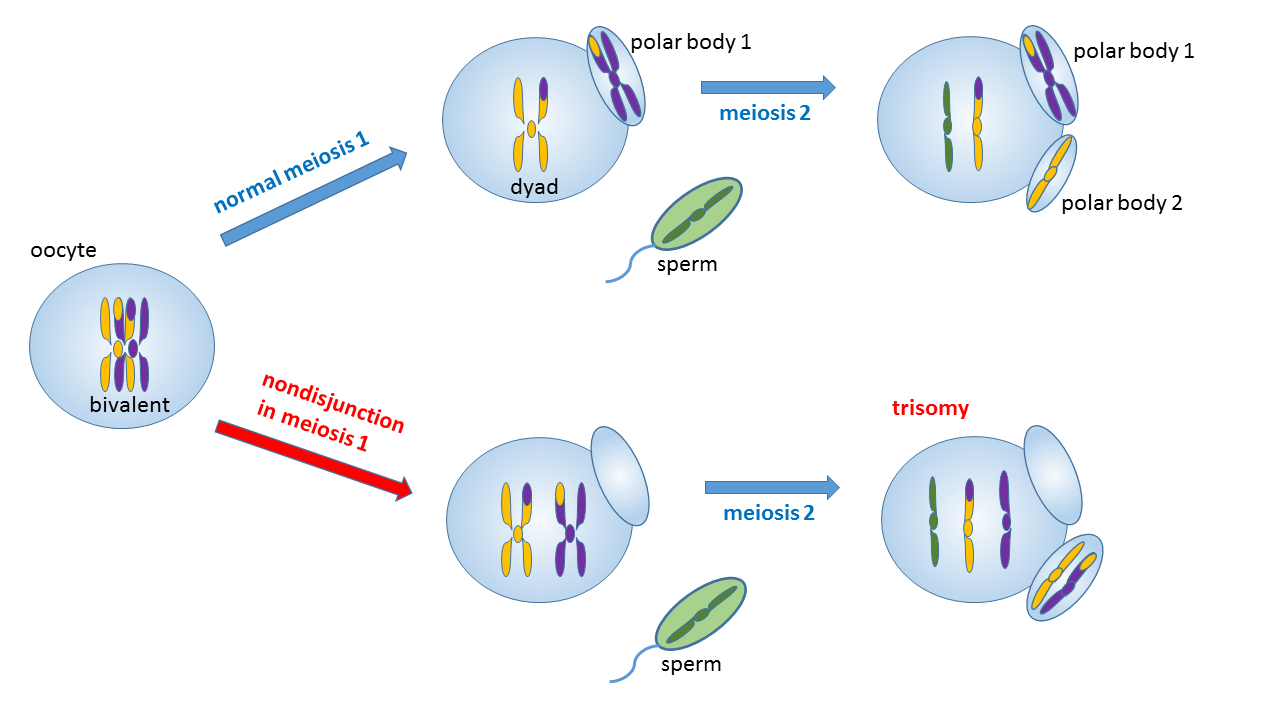
One way an error in meiosis can cause trisomy
Having a baby used to be like opening a surprise package. You didn’t know anything about the baby until it was born. The obstetrician or midwife would announce “It’s a boy” or “It’s a girl”, and everyone would superficially check the newborn to see if everything looked OK. “Ten fingers, ten toes… she’s perfect!” There were things that wouldn’t be obvious right away, like a congenital heart defect. And Down syndrome might not be noticed until later.
Today, unless they choose to wait and be surprised, parents know early in the pregnancy whether the fetus is male or female. You may have been amused (or irritated) by the proliferation of videos of gender reveal parties gone awry. Back in 1982, in my first pregnancy, I was classified as an “elderly primigravida” (primigravida means I had never been pregnant before, elderly denotes an age over 35). At 37, my age put me in the high-risk group for Down syndrome, so they did an amniocentesis to rule that out; it also showed that the fetus was a girl, so we knew the sex early on. My husband delighted in introducing us. He would say, “This is my wife Harriet.” Then he would point to my bulging belly and say, “And this is our daughter Kristin”. Gender reveals are now common, but they can occasionally be wrong. My niece was told she was having a boy; she was surprised by the birth of her daughter.
Prenatal screening for chromosome abnormalities like Down syndrome is a welcome development, but false positives and false negatives are still possible.
Aneuploidy
Science has come a long way during my lifetime. It wasn’t until 1956, when I was 11 years old, that scientists discovered how many chromosomes humans had (23 pairs for a total of 46). Then they figured out that errors in cell division could result in “aneuploidy” where the numbers were larger or smaller than 46, and that Down syndrome was caused by just such an aneuploidy, with an extra copy of chromosome number 21.
Some aneuploidies are incompatible with life and are eliminated by spontaneous abortion. For babies that survive, each aneuploidy is associated with a number of characteristic abnormalities, such as mental impairment, umbilical hernia, malformed ears, webbed toes, heart defects, and many more. Some of these signs are only of cosmetic concern, but others result in severe disabilities, and life expectancy may be decreased.
Down syndrome is also called trisomy 21, and there are other trisomies with three copies of one of the 23 chromosome. In trisomy 18, also known as Edwards syndrome, only 5-10% survive beyond the age of one year. In trisomy 13, also known as Patau syndrome, 90% die in the first year, and those that survive are severely disabled. The average lifespan for Down syndrome has risen to 60 years because of better care.
Chromosome abnormalities can also occur in the sex chromosomes. Usually a female has two X chromosomes (XX) and a male has one X and one Y (XY). In Klinefelter syndrome a male has an extra X chromosome and is XXY. In Turner syndrome a female has only one X chromosome (X0). Other variants are possible, such as XXX and XYY, and mosaicism is also possible, where two different genetic types occur in throughout a single individual’s tissues.
Scientific progress continued apace. The next development was figuring out how to test for aneuploidy before birth. A recent article in American Family Physician reviews the tests that are currently available to screen for aneuploidy. The risk of Down syndrome increases with maternal age, from one in 1480 at age 20 to one in 85 at age 40. But it can occur at any age, so the AFP authors recommend that all pregnant women should be offered aneuploidy screening regardless of their age. But the testing is not perfect. Results can be wrong, and there are ethical issues to consider. Several kinds of testing are currently available.
Preimplantation genetic screening
During in-vitro fertilization, the doctor can biopsy the part of the embryo that will become the placenta. There can be false positives and negatives, since mosaicism can occur and aneuploidy might be present in the placenta or the embryo but not in both. So even women who have had pre-implantation screening can be offered further testing.
First-trimester screening
This testing can be offered after 10 and before 14 weeks’ gestation. It combines ultrasound with two blood tests. Abnormal nuchal transparency can be detected on ultrasound; it predicts structural anomalies and should be followed by detailed ultrasounds at 18 to 22 weeks’ gestation. It is combined with blood tests for maternal serum pregnancy-associated plasma protein A (PAPP-A) levels and human chorionic gonadotropin (hCG) levels. 5% of results will be reported as positive, but most of these will be false positives.
Second-trimester screening
Second-trimester quadruple (quad) screening can be offered after 15 and before 23 weeks’ gestation. It consists of four tests on maternal blood: alpha fetoprotein, unconjugated estriol, hCG, and inhibin A. It can detect 81% of trisomy 21 cases, but as with first-trimester testing, 5% of tests are reported as positive and most of them are false positives.
Combination first- and second-trimester screening
Various forms of combined testing are available to improve the detection rate. In integrated testing, abnormal first-trimester results are withheld from patients until after quad screening. In serum integrated screening, there is no need for a specialized ultrasound technician. In stepwise sequential testing, women whose first-trimester results indicate high risk are offered early invasive diagnostic testing. In contingent sequential testing, low risk women don’t get the second-trimester tests.
Cell-free DNA testing
This is a blood test done after 10 weeks’ gestation. Fragments of placental DNA are circulating in maternal blood. This DNA is amplified to determine if equal amounts are present from each chromosome. This test offers the best sensitivity for the detection of Down syndrome, greater than 99%. It has fewer false positives and higher positive predictive values for trisomies 18 and 21, and it also detects fetal sex and sex chromosome aneuploidy. Three cell-free DNA tests are currently on the market with prices ranging from $795 to $1,400.
Invasive diagnostic testing
If results of aneuploidy screening tests are positive, the next step is counselling and offering invasive testing. There are two kinds of invasive diagnostic test. Chorionic villus sampling tests tissue obtained from the placenta through the cervix or through the abdomen. In amniocentesis, a needle is inserted into the amniotic fluid with ultrasound guidance. Fetal cells are obtained, grown in tissue culture in the lab, and karyotyped to evaluate the chromosomes. With both of these procedures, there is a risk of pregnancy loss: one in 455 for chorionic villus sampling, and one in 900 for amniocentesis.
Ethical issues
It would seem that the only reason for prenatal screening would be to prevent the birth of babies with serious birth defects, although one could also argue that there are advantages to being prepared ahead of time for the birth of a child with special needs. Many women would choose to have a therapeutic abortion after a positive test, but some women have strong moral or religious objections to abortion, equating it to murder. Those women would refuse to terminate a pregnancy for any reason, so there is no point in testing them. And women who would consider abortion need to understand that there can be false negative and false positive results, so there is a possibility that they might abort a fetus that would have been a normal child or that they might have an affected child even after a normal test. If they are comfortable with that small risk, they still might refuse invasive testing because of the greater risk of pregnancy loss. To give informed consent to testing, they must be fully informed, and counselling is helpful.